
Launched in 1952
India was the first country in the world to launch a program for population stabilization
In beginning:
1. Few clinics
2. Training the personnel for above activities
3. Research for contraceptive methods, communication strategy, behavior change etc.
During the period of next 2 five yr. plans i.e.1961-66 & 66-69
FP declared: ‘very center of planned development’
Emphasis shifted from purely clinical approach to ‘Extension education approach’ (more vigorous) for:
• Informing general population about the hazards of ‘Population explosion’ and
• Motivating the people to accept the ‘small family norm’
Lippes loop was introduced in 1965.
The resulting optimism led to creation of a separate Dept. of F. Planning in 1966
• Within the Ministry of Health
The Next 5 yrs. plan (1966 – 1969) brought the strengthening of Family Planning infrastructure in the country.
I.e. at all levels like Primary Health Centers, Sub- Centers, urban FP centers, dist. bureaus, state bureaus etc.
In 1969 – 74, the population explosion was still a threat; hence controlling it was given ‘top priority’
FP program integrated with MCH activities of PHC and S/Cs
I.e. Instead of separate clinics for FP services, these would be delivered at the MCH (Maternal & Child Health) clinics 
1970 – All India Hospital Postpartum Program introduced
1972: MTP Act introduced
Major Changes occurred in 1975 – 80
In April 1976: first National Population Policy came out
• The forcible sterilization campaign which followed, met with widespread disapproval of the public and
• Led to the defeat of the ruling party in 1977
The new Govt. that formed in 1977 formulated a new population policy
• It ruled out any kind of compulsion or coercion for sterilization surgeries forever
• The term ‘Family Planning’ was replaced with ‘Family Welfare’
Ministry of FP – renamed as FW
In the same period, ‘Rural Health Scheme’ (1977) was launched for healthcare of community
It incorporated local people e.g. health guides, trained dais, opinion leaders etc. for general healthcare of their communities.
It was hoped that the Family planning information and services would also get more widespread coverage through the scheme
Shortly, Primary Health Care strategy was adopted by countries at Alma Ata Declaration in 1978: for achieving Health for All (HFA) by 2000 AD
• Through Primary Health Care (PHC) approach
This instrumented the formulation of The National Health Policy in 1982; for achieving HFA by means of Primary Health Care approach
The entire health care delivery system was to be restructured on lines of PHC approach
With Family Planning as important part
Some of the goals of the Health Policy were related to control of fertility
- Long term goal NRR = 1 by 2000
- Birth rate of 21/1000 population
- Death rate of 9/1000 population
- CPR 60%
It became clear by now that ‘Family Planning’ has to be a part of ‘Primary Health Care’
Reducing birth rates: Cannot be achieved by promoting family planning schemes
It was seen that the populations with better
o Healthcare systems
o Health indicators and
o Education and development indicators
Automatically had lower birth rates
Probably it is the conviction among populations that most of the offspring will get the opportunity to develop into healthy adults which encourages adoption of ‘small family norm’.
Hence it was realized that improving the health and status of Children, women and families may automatically raise acceptance of the small family norm
Hence focus shifted towards Programs for Improving Health of Mothers & Children e.g.
Universal Immunization (1985 – 86) for reduction of mortality and morbidity among infants and young children due to VPDs
Oral Rehydration Therapy (ORT) started for reduction of high mortality due to diarrhea
As dehydration from diarrhoea was a leading cause of mortality in children
All these programs were later integrated under a common program k/a the CSSM (Child Survival & Safe Motherhood) program in 1992
Later (1994), reproductive health was introduced and the program was renamed as into RCH (Reproductive & Child Health) program, which was for addressing health of
Women in reproductive age group (15 – 49 yr.)
Mothers
Children
Adolescents
(Integration: the purpose is to prevent overlapping of efforts and expenditure)
National Population Policy 2000 was released for promoting Family Welfare activities.
Currently: the ‘National Family Welfare Program’ which has two components:
1. RCH program: for health of
Children
Adolescents
Women
Pregnant women and
Lactating mothers
2. Family Planning program focusing on population stabilization
Contraceptives
Safe abortion services
Schemes & legislation for promoting small family norm
IEC etc.
Organization of NFWP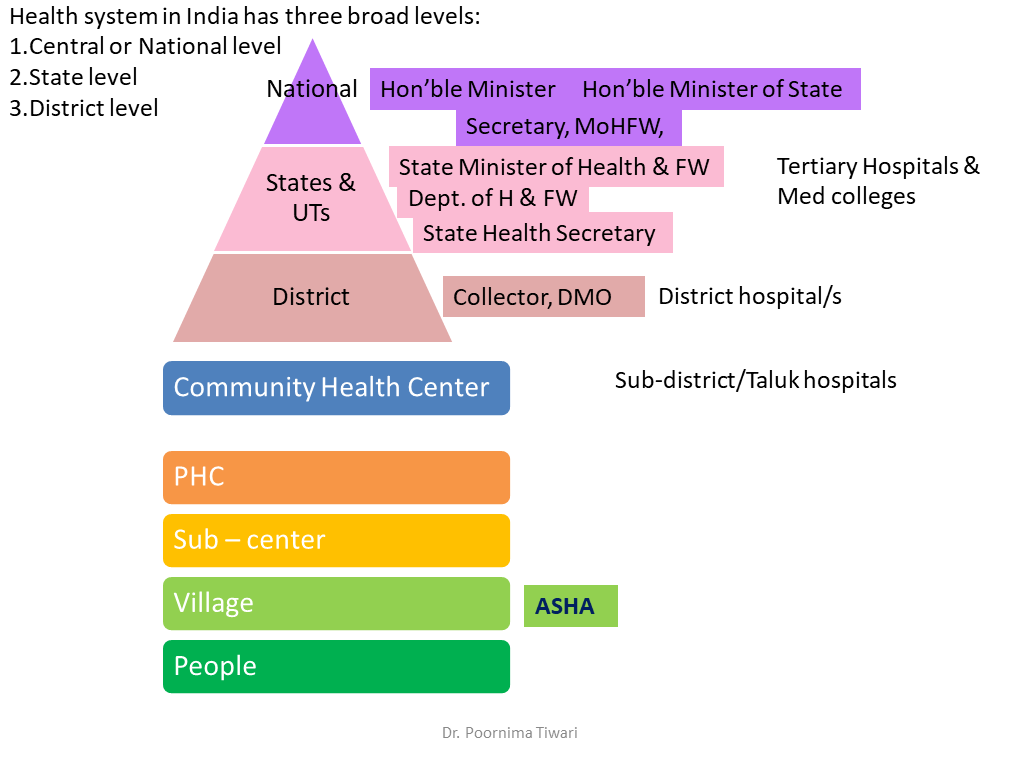
As per the latest development all health related programs have been integrated under the umbrella program of ‘National Health Mission’ (NHM)
1. National Rural Health Mission (NRHM) launched in 2005
2. Next came the ‘National Urban Health Plan’
These were also then merged into NHM
More strategies for promoting the health of vulnerable family members keep getting introduced e.g.
2014: India Newborn Action Plan (INAP); with an aim to attain a single digit NNMR (Neo-natal mortality rate) by 2030
2015: RMNCH + A strategy launched for providing a continuum of care for different stages of life
2017: new National Health Policy launched
Reference:
Demography and Family Planning. In Park’s Textbook of Preventive & Social Medicine editor: K.Park. 26th ed. Bhanot Publications, Jabalpur, India
Demography, Family Welfare Planning and Contraception. In. Textbook of Community Medicine, 4th ed. Editor: Rajvir Bhalwar. Wolters Kluwer Lippincott, Gurugram, India