Essential Newborn Care: Immediate Care, Examination & Risk Identification
Objective
• To assist the newborn in adaptation to the extra-uterine environment
This involves the following:
1. Cardio – respiratory function: Initiation of respiration and oxygenation of blood
2. Body temperature maintenance
3. Feeding establishment
4. Infection prevention
5. Early detection and management of:
• Congenital disorders
• Other disorders
• Infection
Essential newborn care comprises of following actions:
1. Immediate care
2. Neonatal examinations
3. Identifying ‘high – risk’ infants
1. Immediate care - at Birth
1. Clearing the airway
2. APGAR score
3. Care of the cord
4. Care of the eyes
5. Care of the skin
6. Body temperature maintenance
7. Breast feeding initiation and establishment
• Preparing for birth
Make sure that the following materials/conditions are available for the newborn
1. Two clean and warm towels for thermal protection of the baby
a. One for drying and wrapping the baby initially,
b. The other for covering the newborn to prevent heat loss
2. A draught-free delivery room with a temperature of at least 25 °C
3. Soap, water, clean gloves, cotton, gauze and a clean labour table for delivery to ensure the six "cleans"
a. Clean hands,
b. Clean surface,
c. Clean cord cut,
d. Clean cord tie,
e. Clean cord stump and
f. Clean perineum
4. A clean delivery kit for cord care
5. Self-inflating bags (two, of a size appropriate for a newborn) and masks (sizes zero and one) for resuscitation
6. A suction device (mucus extractor)
7. A radiant heater
8. A blanket
9. A clock/watch to note the time of delivery
Clearing the Airway
Establishment and maintenance of breathing is the most important immediately after birth, everything else is secondary
• The airways should be cleared of mucus and other secretions
– Positioning the baby with his head low may help in drainage of secretions
– Gentle suction to remove mucus and amniotic fluid also helps
• If natural breathing fails to establish within a minute of birth, resuscitation is necessary
1. Suction and
2. Assisted respiration
• Application of oxygen mask
• Intubation
• All labor wards should be equipped with resuscitation equipment including oxygen
• If there is no gasping or breathing at all even after 20 minutes of effective ventilation (and cardiac massage, if required), stop ventilation
Care of the cord
• In a normal neonate: Cut and tie the cord when it stops pulsating
– The advantage is that the baby derives about 10 ml of extra blood, if the cord is cut after pulsation ceases
– Using properly sterilized instruments and cord ties
• Do NOT apply anything on the stump; keep the cord clean and dry.
• Inspect the cord for bleeding 2 hours after ligation
• Inspect for discharge or infection till healing occurs.
• The cord should be kept as dry as possible
• It dries and shrivels up and separates by aseptic necrosis in 5 – 10 days
Maintaining the body temperature
• The normal body temperature of a newborn is between 36.5 to 37.5 ⁰C
• Hypothermia is a body temperature of <36 °C
• A newborn baby is projected out of warm womb of the mother into an environment which may be 10 to 20 ⁰C
• A newborn has little thermal control and can lose body heat quickly
• Immediately after birth, most of the heat loss occurs through evaporation of the amniotic fluid from the body of the wet child
• As much as 75% of the heat loss can occur from the head
• Hypothermia results in:
– increased oxygen consumption; hence hypoxaemia,
– increased glucose consumption; hence hypoglycaemia and metabolic acidosis.
– Hypoxaemia and hypoglycemia can result in the death of the newborn
– Among survivors, it can lead to permanent impairment of the brain resulting in developmental handicaps
• Receive the baby in a dry, warm, clean towel.
• Dry the baby well
• Discard the wet towel Immediately and
• Wrap/cover the baby (except for the face and upper chest) in a fresh, warm, clean and dry towel.
• The baby should be kept wrapped during the assessment and suction ventilation applied (if required)
• Place the baby near a source of warmth.
– A normal baby, who is crying well after birth, can be placed in skin-to-skin contact with the mother's abdomen and covered with a dry cloth.
– additional heat can be provided by placing the baby under a source of heat such as
• a lamp with a 200 Watt bulb or
• under a radiant warmer
• Practices such as separating the baby from the mother for the first 12 – 24 hours of life are harmful
• Pre term and low birth babies lose heat more easily through their skin as they have less subcutaneous fat for insulation
• Ensure that during and after the delivery, no fans are running in the delivery room, and no windows are open through which air currents blow into the room
Care of the skin
• Clean the blood, mucus and meconium on the newborn's body before presenting it to the mother
• Bathing the newborn soon after birth is not recommended as it causes a drop in the body temperature
– discourage the mother from giving bath to the baby during the first day after birth.
– The mother or the attendant can clean the baby by wiping with a soft moist cloth.
– When the baby is given a bath, bathing should be done
• quickly
• in a warm room,
• using warm water.
• Low birth weight infants should not be given a bath
– Blood, meconium and some of the vernix will have been wiped off during drying at birth.
– The remaining vernix does not need to be removed as it is harmless
– If cultural tradition demands bathing, this should not be carried out before 6 hours after birth, and preferably on the second or third day of life as long as the baby is healthy and its temperature normal
Care of the eyes
• The eyes should be cleaned
– at birth and
– once every day
• using sterile cotton swabs soaked in
– sterile water or
– Normal saline.
• From inner to the outer side
• Each eye should be cleaned using a separate swab.
• The routine use of local antiseptic drops for prophylaxis is not recommended
– The earlier practice of instilling a drop of freshly prepared silver nitrate solution (1%) to prevent gonococcal conjunctivitis is no longer recommended
Breast Feeding - Initiation and Establishment
• Breast feeding should be initiated within one hour of birth
• If suckling is poor, ensure correct positioning and attachment of the baby to the breast
• Although there is little milk at this time, it helps to establish
– feeding and
– a close mother child relationship known as ‘bonding’
– The first milk is called colostrum and is the most suitable food for the baby during this early period because it contains a high concentration of
– protein and other nutrient the body needs
– anti-infective factors which protect the baby against respiratory infections and diarrheal diseases
• Supplementary feeds are not necessary, not even water
• The regular milk comes on the third to sixth day after birth
• The baby should be allowed to breast feed whenever it wants
– This is k/a ‘feeding on demand’
– Feeding the baby on demand helps the baby to gain weight
• It is very important to advise mother to avoid feeding bottles
APGAR score
• Taken at 1 minute and again at 5min
• If Apgar scoring is omitted, it is considered as negligence
APGAR score is calculated by careful observation of the following signs:
1. Heart rate
2. Respiration
3. Muscle tone
4. Reflex response and
5. Color of the infant
• Each sign is given a score of 0, 1 or 2
• It provides an immediate estimate of the physical condition of the baby
• A perfect score is 9 or 10
• An Apgar score of >7 is considered satisfactory
• 4 – 6 indicates moderately depressed
• 0 – 3 indicates severely depressed baby
• A score below 5 needs prompt action
• Infants with low Apgar scores at 5 minutes of age are subject to a high risk of complications and death during the neonatal period
Suggested mnemonic:
Activity for muscle tone
Pulse for heart rate
Grimace for reflex response
Appearance for skin colour
Respiration for breathing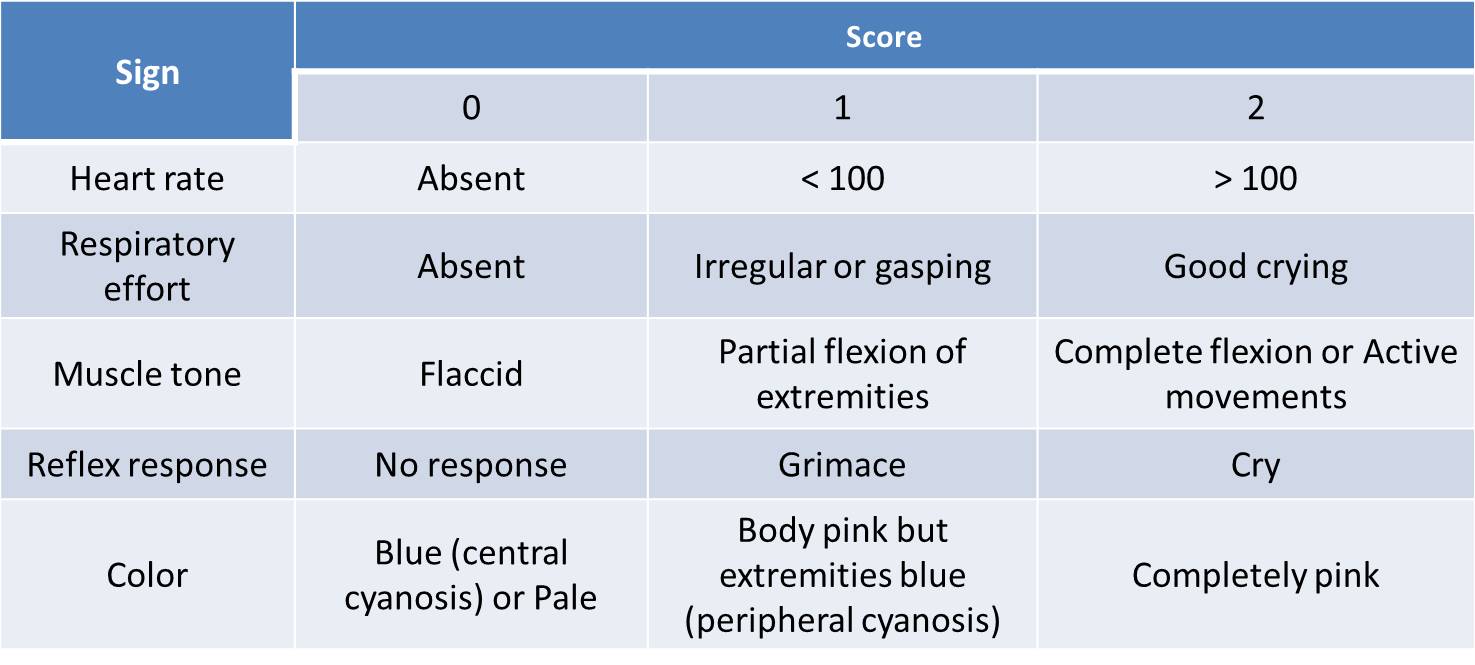
Neonatal examinations
First examination
Made soon after birth and preferably in the delivery room
This examination is:
– To ascertain that the baby has not suffered injuries during the birth process
– To detect malformations especially those requiring urgent treatment and
– To check for danger signs
– Birth weight
– Should preferably be taken within first hour of life
– The naked baby should be placed on a clean towel on the scale pan
– Home deliveries: place the baby in a sling bag for using a salter weighing scale
– The child is weighed to the nearest 100 gm
2. Length
– With a measuring board (infantometer)
– Fixed head piece
– Infant lies supine with
– Legs fully extended and
– Feet flexed at right angle to lower legs
– Two people are needed to hold the baby correctly
– The sliding board is moved firmly against the feet before the reading is taken
– Length is taken to the nearest 0.1 cm
• The length may be taken within first 3 days if not possible to take immediately at birth
• Head Circumference
• Use a tape measure at the maximum circumference of the head in occipital frontal diameter
• The purpose is
• To assess the baby’s size against known standards for the population
• To compare the size with estimated period of gestation
• To provide a baseline against which subsequent progress can be measured
• The measurement may change slightly during the first 3 days owing to moulding during labour
• The following abnormalities found on examination should be immediately attended to:
• Cyanosis of the lips and skin
• Any difficulty in breathing
• Imperforate anus
• Persistent vomiting
• Sighs of cerebral irritation s/a
• convulsions
• Neck rigidity
• Bulging of anterior fontanel and
• Temperature instability
Second Examination
This should be made preferably by a pediatrician within 24 hours after birth
This examination should form the first stage of a continual process of health care surveillance
It is a detailed systematic examination from head to foot, conducted in good light
The following protocol will be found useful for such an examination
Body size
• Body weight
• Crown heel length
• Head and thoracic perimeters
Body temperature
Skin
• Cyanosis of lips and skin
• Jaundice
• Pallor
• Generalized erythema
• Vesicular and bullous lesions
Cardio respiratory activities
• Cardiac murmurs
• Absence of femoral pulse
• Central cyanosis
• RR >60
• Thoracic cage retraction on inspiration
Neuro behavioral activity
• Posture
• Neck retraction
• Frog like posture
• Hyper extension of all limbs
• Hyperflexion of all limbs
• Asymmetrical posture
Muscle tone
• Tendon reflexes
• Cry
• Movements
Head and face:
Hydrocephalus:
• Large fontanelles
• Prominent scalp veins
Eyes:
• Cataract
• Coloboma
• Conjunctivitis
Ears:
• Dysmorphism
• Accessary auricles
• Periauricular pits
Mouth and lips:
• Hare lip & cleft palate
Abdomen:
• Sighs of distension
• Abnormal masses
• Imperforate anus
Limbs and joints:
• Deformities
• CDH
• Extra digits
Spine: NT defects
External genitatlia:
• Male:
o hypospadias
o Undescended testis
o Hydrocele
• Female:
o Fused labia
o Enlarged clitoris
References:
• Preventive Medicine in Obstetrics, Pediatrics and Geriatrics, Park’s Textbook of Preventive and Social Medicine: 23rd edition, 2015
• Maternal Health Division, Department of Family Welfare, Ministry of Health & Family Welfare, Government of India: August, 2005. Guidelines for Pregnancy Care and Management of Common Obstetric Complications by Medical Officers. Available on, http://jknrhm.com/Guideline/Normal_delivery_and_management_of_obstetric_... downloaded on 20th Dec 2016
• Maternal Health Division, Department of Family Welfare, Ministry of Health & Family Welfare, Government of India: August, 2009, TRAINEES' HANDBOOK for TRAINING of Medical Officers in Pregnancy Care and Management of Common Obstetric Complications. Available on, http://tripuranrhm.gov.in/Guidlines/Pregnancy_Care.pdf downloaded on 20th Dec 2016
Risk identification in newborn: http://www.ihatepsm.com/blog/risk-identification-newborn
http://www.ihatepsm.com/blog/essential-newborn-care
Antenatal Care: http://www.ihatepsm.com/blog/antenatal-care
Components of Antenatal Care: http://www.ihatepsm.com/blog/components-antenatal-care
Prenatal Advice: http://www.ihatepsm.com/blog/prenatal-advice
Risk Approach in Antenatal Care: http://www.ihatepsm.com/blog/risk-approach-antenatal-care
Ensuring Complete Registration of Antenatal Women in the Jurisdiction: http://www.ihatepsm.com/blog/ensuring-complete-registration
Specific Health Protection during Antenatal Visits; http://www.ihatepsm.com/blog/specific-health-protection-during-antenatal...
Lecture on Antenatal Care: http://www.ihatepsm.com/resource/antenatal-care
5-Page ANC History Taking Format: https://ihatepsm.com/blog/5-page-anc-history-taking-format-essential-gui...
Pallor and its Grading: https://ihatepsm.com/blog/pallor-and-its-grading
Why ANC History Taking Matters?: https://ihatepsm.com/blog/why-anc-history-taking-matters
#Obstetric index (GPAL) in Antenatal Case History: https://ihatepsm.com/blog/obstetric-index-gpal-antenatal-case-history
#Decoding Gravida and Para: Terms in Antenatal History Taking: https://ihatepsm.com/blog/decoding-gravida-and-para-terms-antenatal-hist...
#Duration of Pregnancy: Understanding the Trimesters and Gestational Age Categories: https://ihatepsm.com/blog/duration-pregnancy-understanding-trimesters-an...
#Calculation of Expected Date of Delivery (EDD) and Period of Gestation (POG): https://ihatepsm.com/blog/calculation-expected-date-delivery-edd-and-per...
#Antenatal Care and Case Booking: https://ihatepsm.com/blog/antenatal-care-and-case-booking
#Clinical Significance of Antenatal History Components (Socio-Demographic components): https://ihatepsm.com/blog/clinical-significance-antenatal-history-compon...
Antenatal History Taking: Significance of Clinical Components: https://ihatepsm.com/blog/antenatal-history-taking-significance-clinical...
Trimester-wise History Taking in Antenatal Care: FIRST Trimester: https://ihatepsm.com/blog/trimester-wise-history-taking-antenatal-care-f...
Trimester-wise History Taking in Antenatal Care: SECOND Trimester: https://ihatepsm.com/blog/trimester-wise-history-taking-antenatal-care-s...
Trimester-wise History Taking in Antenatal Care: THIRD Trimester: https://ihatepsm.com/blog/trimester-wise-history-taking-antenatal-care-t...
Trimester-wise History Taking in Antenatal Care: A Comprehensive Guide (all 3 trimesters): https://ihatepsm.com/blog/trimester-wise-history-taking-antenatal-care-c...
Components of Birth Preparedness and Complication Readiness (BPCR): https://ihatepsm.com/blog/components-birth-preparedness-and-complication...
BPCR in brief: https://ihatepsm.com/blog/%E2%80%98birth-preparedness-and-complication-r...
Specific Health Protection during Antenatal Visits: https://ihatepsm.com/blog/specific-health-protection-during-antenatal-vi...